Reversing Cognitive Decline: The Truth Is Out
[lwptoc]
[separator top_space=”20px” bottom_space=”20px”]
Welcome to my blog ‘Reversing Cognitive Decline’.
You may like to check out the section of my blog dedicated to Alzheimer’s disease: click here. Posts include:
- Inhalation Alzheimer’s: A Treatable Epidemic
- Infra red light and methylene blue: the perfect combo.
- Can psychedelics help Alzheimer’s?
- Nutritional Status Helps Prevent Alzheimer’s.
- The Three Sub-types of Alzheimer’s.
The pathobiology of Alzheimer’s disease dictates a system or program rather than a single targeted agent.
Reversing Cognitive Decline
The basic tenets for such a comprehensive therapeutic system are described in the paper (1) as:
- Just as for other chronic illnesses such as atherosclerotic cardiovascular disease, the goal is not simply to normalize metabolic parameters, but rather to optimize them. As an example, a serum homocysteine level of 12 μmol/l is considered to be within normal limits, but is well documented to be suboptimal.
- Based on the hypothesis that AD results from an imbalance in an extensive plasticity network, the therapy should address as many of the network components as possible, with the idea that a combination may create an effect that is more than the sum of the effects of many monotherapeutics
- Just as for other chronic illnesses such as osteoporosis, cancer, and cardiovascular disease, the underlying network features a threshold effect, such that, once enough of the network components have been impacted, the pathogenetic process would be halted or reversed. Therefore, even though it is not expected that most patients will be able to follow every single step of the protocol, as long as enough steps are followed to exceed the threshold, that should be sufficient.
- The approach is personalised, based on the contributory laboratory values affecting the plasticity network; and is computationally intensive, since many physiological data points are analysed, interdependent network-component status is assessed, and many interventions are prioritised to determine the therapeutic program.
- The program is iterative, so that there is continued optimisation over time.
- For each network component, the goal is to address it in as physiological a way, and as far upstream, as possible.
In Alzheimer’s disease, there is a fundamental, age-associated imbalance between the dynamically opposed physiological processes that mediate plasticity, i.e., between synaptoblastic and synaptoclastic activity.
This therapeutic system is summarised in the paper:
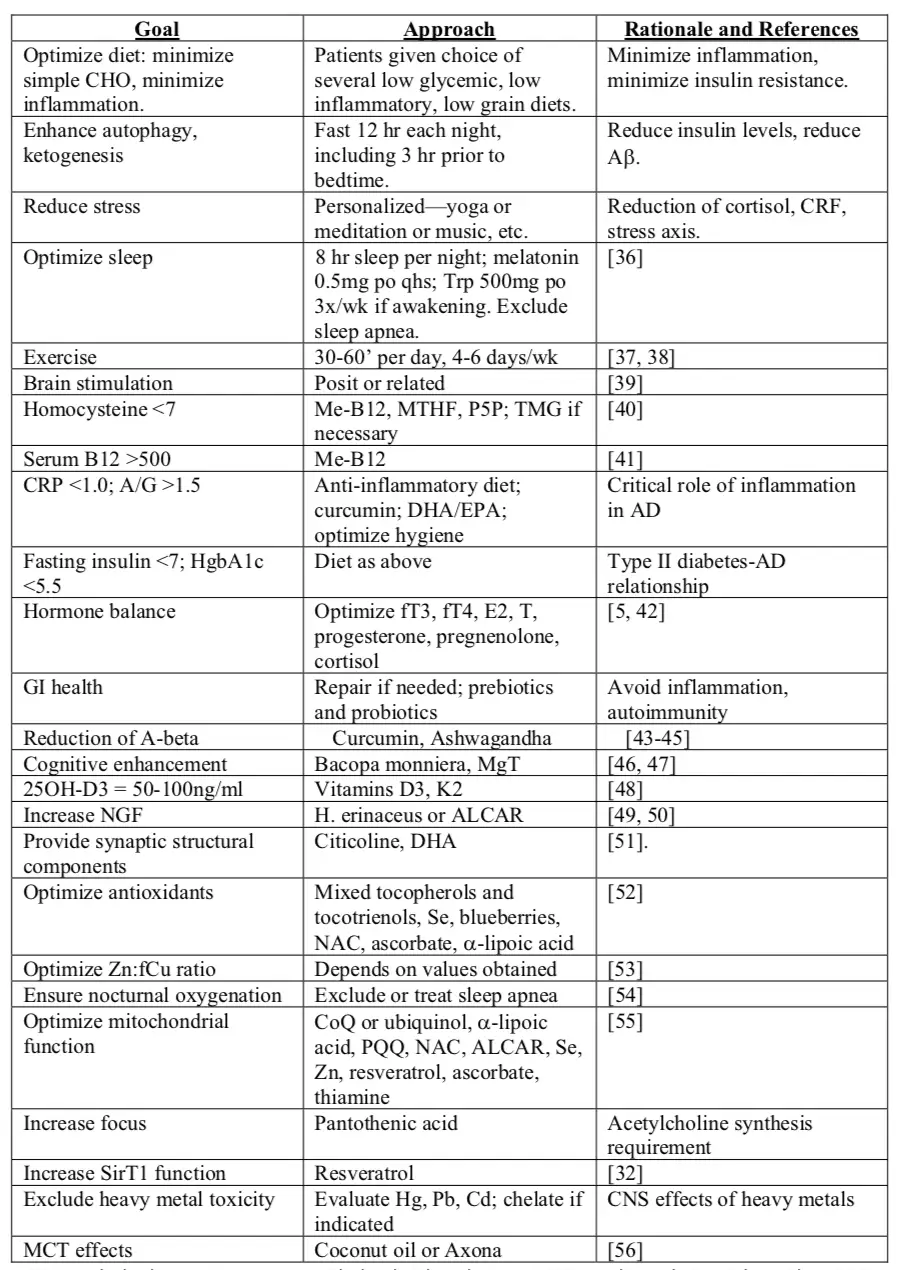
The Evidence
Results from the 10 patients reported in this paper suggest that memory loss in patients with subjective cognitive impairment, mild cognitive impairment, and at least the early phase of Alzheimer’s disease, may be reversed, and improvement sustained, with the therapeutic program described here. Reversing cognitive decline is possible!
The author stressed that, at the time (2016), “this is the first such demonstration. However, at the current time the results are anecdotal, and therefore a more extensive, controlled clinical trial is warranted.” (1)
The results reported here are compatible with the notion that metabolic status represents a crucial, and readily manipulable, determinant of plasticity, and in particular of the abnormal balance of plasticity exhibited in subjective cognitive impairment, mild cognitive impairment, and early AD. (1)
References:
- Metabolic profiling distinguishes three subtypes of A.D (click here)