Mast Cell Activation Syndrome And The Gut
Welcome to my blog on Mast Cell Activation Syndrome And The Gut. You may like to check out my section of the blog all on histamine.
What Is Mast Cell Activation Syndrome?
Mast cell activation syndrome (MCAS) is a chronic multi-system disease of abnormal mast cell (MC) activation leading to inflammatory and allergic symptoms (1).
How Do You Know You Have Mast Cell Activation Syndrome?
This syndrome can be diagnosed by the medical history and measurable biomarkers. These will be discussed below under the test section.
It is worth knowing that liver involvement in MCAS may be present. In fact…
44% of MCAS patients had mildly increased liver chemistries, especially during a symptom flare in a study of 56 patients. (1)
Tests For Mast Cell Activation Syndrome
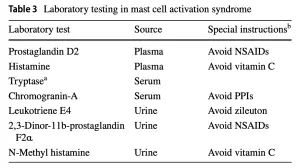
Mild elevations in tryptase can be helpful in diagnosing MCAS; however, a normal tryptase level does not exclude MCAS. Trypase is tested for in the blood by various private companies.
Because tryptase isn’t a great biomarker for MCAS, we need to also consider other biomarkers of mast cell activation. Two options are:
- Leukotriene E4 (which can be tested in urine)
- Heparin (which can be tested for in plasma)
Heparin is also not the best of markers. The problem here is that many commercial laboratories do not have sensitive assays (tests) for endogenous heparin.
Prostaglandin D2 (plasma) appears to be a sensitive and relatively specific mediator in MCAS.
Chromogranin A is another commonly elevated mediator and is easily measured in serum. However, increased chromogranin A levels can be seen in heart, kidney, or liver failure, active or recent proton pump inhibitor use, chronic atrophic gastritis, and the rare neuroendocrine malignancies (1).
To complicate things further, both plasma and urine mast cell mediators (such as the above biomarkers) are unstable at room temperature or higher, thus requiring stringent specimen collection and handling protocols (i.e., chilled centrifugation and frozen storage and transportation). Urine collection is generally performed for 24 h, and the collection container(s) should be kept either on ice or in a refrigerator, then transported on ice to the laboratory, and frozen for transportation to the testing laboratory (1). Not ideal for a busy person!
Mast Cell Activation Syndrome And The Gut
It’s important to point out that mast cells play integral parts in normal gut physiology (2). As is so often the case, we need the right amount of histamine for optimal function.
But it’s also important to know that the mast cell has only recently been recognised as a major player in our specialty – it is perhaps one of the most missed diagnosis in my opinion!.
Mast cell activation syndrome is thought to be a common, yet under-recognised, chronic multi-system disorder caused by inappropriate mast cell activation. Gastrointestinal symptoms are frequently reported by these patients and are often mistaken by physicians as functional gastrointestinal disorders.
In a study of 20 refractory IBS patients, 19 had MC symptoms and 11 of 12 studied for MC mediators had positive results (1)
MCAS is often associated with hypermobile Ehlers–Danlos syndrome (hEDS) and postural orthostatic tachycardia syndrome (POTS), both of which also have extensive GI system involvement (1).
What Is The Prevalence Of MCAS In Those With Gut Issues?
We’ve already quoted a paper saying that mast cell activation syndrome may be quite common, but how common?
Well a recent study looked at this. The researchers looked at 2083 functional gastrointestinal disorders patients. Functional dyspepsia (FD) was diagnosed in 1214 patients (58%), IBS in 47 (2%), overlapping IBS and functional dyspepsia in 625 (30%) and 197 (9%) had neither FD nor IBS (3).
Using the cut-off of symptoms from two or more organ-systems, MCAS existed in:
- 1773 (85%) of all 2083 FGID patients.
- In 1033 (85%) with FD.
- 36 (76%) with IBS.
- 557 (89%) with overlapping IBS and FD.
- 147 (75%) without IBS/FD
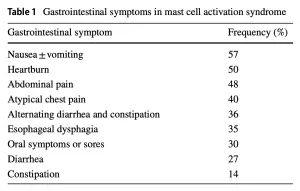
What Are Gut Specific Symptoms Of Mast Cell Activation Syndrome?
Gastrointestinal disorders from mast cell mediators often present with apparent irritable bowel syndrome, dyspepsia, chronic or cyclical nausea, and heartburn.
What Triggers Mast Cell Activation In the First Place?
Triggers for mast cell activation include stress, food, alcohol, excipients in medications, infections, altered microbiome, and environmental stimuli including heat, chemical, and mould exposure (1).
What Is The Normal Function Of Mast Cells?
Mast cells are multifunctional immune cells which play crucial roles in innate and adaptive immunity.
I always use the example of the scene in the movie ‘Hitch’ with Will Smith whereby after eating some shel fish we see him in the pharmacy looking for anti-histamines with an eat and lip the size of a golf ball.
Mast cells distribute into all vascularised tissues, preferentially residing at environmental interfaces, such as mucus membranes and mucosal layers of the GI, respiratory, and urinary tracts
Mast cells participate in host defence, tissue repair, wound healing, and angiogenesis. Mast cells react to allergens, tissue trauma, and infection and quickly respond by releasing biologically active mediators from both intracellular stores and by delayed de novo synthesis. Over 200 mast cells mediators have been identified, including (1):
- Biogenic amines (e.g., histamine).
- Proteases (e.g., tryptase and chymase).
- Cytokines (e.g., interleukins and TNF-α).
- Eicosanoids (e.g., prostaglandins and leukotrienes).
- Hheparin.
- Growth factors.
Think of these mediators as stuff the mast cell produces.
Dysbiosis, SIBO, And Mast Cell Activation Syndrome
Changes in the microbiome and intestinal permeability lead to the accumulation and activity of MCs and lympho- cytes within the GI tract. Dysbiosis and small intesti- nal bacterial overgrowth act as stimuli to the mast cells which release mediators that activate lymphocytes. In turn, the T-lymphocytes secrete microparticles which further activate mast cells. The activated mast cells and T-cells secrete cytokines which increase intestinal permeability. This furthers the vicious cycle whereby bacterial and lipopolysaccharide translocation causes inflammation and increased intestinal permeability. The clinical impact is that mast cell degranulation is increased and the overall inflammatory state is increased. When the aberrant MCs of MCAS are present, this magnifies this condition (1).
Diet And Mast Cell Activation Syndrome
Data regarding specific dietary interventions in the treatment of MCAS are lacking, and the most effective dietary inter- vention remains the identification and avoidance of triggers. Histamine, gluten, and dairy-protein-free diets have been recommended on the basis of clinical experience. Elimination diets play an important role in MCAS therapy.
In my experience, high-histamine foods can activate mast cells in the gut causing direct and systemic symptoms (i.e symptoms outside the gut too!). The aberrant mast cells and normal mast cells not only release histamine, but the mast cells have receptors for histamine which then activate other MCs and other cells in the body. High-histamine foods can release histamine which binds to mucosal mast cell receptors on both aberrant and normal mast cells (1).
Gluten (and dairy products) are listed as high-FODMAP foods.
Investigations of the effect of a low-FODMAP diet in IBS-d patients have shown reduction of plasma histamine levels.
Furthermore, high-FODMAP diet in mice results in increased visceral hypersensitivity and increased mast cell density in the colon.
Supplements And Mast Cell Activation Syndrome
Sustained release vitamin C 500 mg daily, vitamin D daily, and quercetin 500 mg to 1000 mg once to twice daily are other over-the-counter interventions sometimes found helpful in MCAS. Vitamin C stabilises MCs by reducing histamine formation and chemical degradation of released histamine. Quercetin is a plant-based flavonoid that inhibits cyclooxygenase and lipoxygenase activity, thereby reducing production of inflammatory mediators such as prostaglandins. Supplementation with vitamin D is dose adjusted according to the serum level and may play a role owing to downregulation of MC receptors (1).
Treatment with probiotics that reduce histamine output are other avenues to explore in the therapy of MCAS.
[separator top_space=”20px” bottom_space=”20px”]
References
- Mast Cell Activation Syndrome: A Primer for the Gastroenterologist PMID: 32328892
- Symptoms of mast cell activation syndrome in functional gastrointestinal disorders PMID: 31687861
- Gastrointestinal Manifestations of Hypereosinophilic Syndromes and Mast Cell Disorders: a Comprehensive Review PMID: 30003499
[empty_separator top_space=”10px” bottom_space=”10px”]
[full_column]
[empty_separator top_space=”10px” bottom_space=”10px”]
[vc_row][vc_column][products_mixed layout=”listing” ids=”6834, 6836, 6831″][/vc_column][/vc_row]